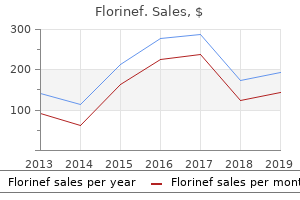
Medical Instructor, University of Minnesota Medical School
Categorical data were described on numbers (percentage) and analyzed by chi-square test gastritis symptoms stomach pain cheap florinef 0.1 mg fast delivery. Continuous data were described as mean +/standard deviation and analyzed using standard t-test gastritis diet ęŕëüęóë˙ňîđ order 0.1mg florinef free shipping. Statistical analysis e) the Gensini score was expressed as the sum of the scores for the all coronary arteries [13] gastritis diet ÷čňŕňü discount florinef american express. Results There was a significant difference between the two groups as regard age chronic gastritis risks florinef 0.1mg without prescription, (P-value <0. There was a significant difference between the two groups as regard Hypertension, Diabetes, and Mitral annular calcification. There was statistically high significant difference between the two groups as regard Gensini score and number of vessel affected. There was statistically high significant difference between the two subgroups as regard Gensini score and number of vessel affected. There was a significant correlation between sum of aortic valve cusps thickness and (age  serum cholesterol level  Gensini score) (P-value <0. Figure 2: Comparison between the two groups according to age Figure 3: Comparison between the two groups according to other parameters. Figure 7: Comparison between the two subgroups according to number of vessels affected. Figure 8: Correlation between sum of aortic valve cusps thickness and Gensini score. Also, Gensini score was of significant difference between the two subgroups compared to the control group (p value < 0. Boon A, Cheriex E, Lodder J, Kessels F (1997) Cardiac valve calcification: characteristics of patients with calcification of the mitral annulus or aortic valve. Lindroos M, Kupari M, Heikkila J, Tilvis R (1993) Prevalence of aortic valve abnormalities in the elderly: an echocardiographic study of a random population sample. Roberto M Lang, Michelle Bierig, Richard B Devereux (2005) Recommendations for chamber quantification. Soydinc S, Davutoglu V, Dundar A, Aksoy M (2006) Relationship between Aortic Valve Sclerosis and the Extent of Coronary Artery Disease in Patients Undergoing Diagnostic Coronary Angiography. Shu-Jian Sui, Man-Yi Ren, Fu-Yu Xu, Yun Zhang (2007) A High Association of Aortic Valve Sclerosis Detected by Transthoracic Echocardiography with Coronary Arteriosclerosis. In the closed position, each leaflet forms a nominal angle of 40Ń” relative to the plane of the orifice. In the open position, the plane of each leaflet forms a nominal angle of 90Ń” relative to the plane of the orifice. This form of sewing ring attachment to the orifice allows for rotation of the sewing ring in situ during implantation. The On-X Prosthetic Heart Valve is available in 3 aortic and 2 mitral sewing ring configurations. Aortic valves, size 19 mm through 25 mm, are designed for intrasupra-annular sewing ring position, while the valve size 27/29 mm is designed for intra-annular sewing ring position. Avoid contacting the carbon surfaces of the valve with gloved fingers or any metallic or abrasive instruments as they may cause damage to the valve surface not seen with the unaided eye that may lead to accelerated valve structural dysfunction, leaflet escape, or serve as a nidus for thrombus formation. Avoid damaging the prosthesis through the application of excessive force to the valve orifice or leaflets. Therefore, the following statement is provided: the implanted On-X prosthetic heart valve is designed for single use only. In addition to the risks listed in Section 5, re-use may cause procedural complications including device damage, compromised device biocompatibility, and device contamination. The standard mitral sewing ring is available in sizes 23, 25, 27/29 and 31/33 mm, while the Mitral Conform-X sewing ring is available in size 25/33 only. Figure 2: Standard or Extended Aortic Valve Holders Extended Holder Standard Holder the dimensional and model specifications for all available sizes of the On-X Prosthetic Heart Valve are shown in Table 1 and Figure 1. The sterility expiration date of the On-X Prosthetic Heart Valve is recorded on the outer package label. The instruments, supplied separately, are provided as a set, which includes sizers, rotators, an instrument handle, and a leaflet probe.
Hemangiomas are vascular tumors characterized by increased cellular proliferation gastritis diet virus buy 0.1mg florinef overnight delivery. Approximately 80% of hemangiomas are noted in the first month of life gastritis diet quizzes cheap florinef 0.1mg with amex, and 60% occur in the head and neck region gastritis diet ulcerative colitis order 0.1mg florinef with visa. May be present at birth (30-50%) but usually appear in the first two weeks of life gastritis diet soy sauce generic florinef 0.1mg otc, with 80% appearing in the first month of life 46 a. Proliferating phase  0-9 months (with most of the growth achieved by 3 months) b. Larger problematic lesions can be treated with medical therapy (oral prednisolone or oral propanolol) c. Lesions (of any stage) that are compromising function or destroying vital structures B. Arise in the fetus, are fully grown at birth, and do not have post-natal growth 2. Red-violaceous with coarse telangiectasias, central pallor, and a peripheral pale halo 3. More common in the extremities, have an equal sex distribution, and are solitary with an average diameter of 5 cm 4. Resection can be considered if the scar will be less noticeable than the lesion C. Presents as a large (>5cm), superficial, and diffuse lesion, with the overlying skin deep red-purple, tense, painful, and shiny 2. Typically involves the trunk and extremities, 50% present at birth (but can appear in childhood) 3. Kasabach-Merritt phenomenon (thrombocytopenia <25,000, bruising, and bleeding) is common 4. Regression seen after age 2, although long-term chronic pain and stiffness can persist 5. Slow-flowing vascular malformation characterized by ectatic vessels located at various levels within the dermis 2. Present at birth, slowly increase in size as the child grows, change size with position, and are prone to thrombosis (phlebolith formation) 3. Most commonly occur in the cervicofacial region, axilla/chest, mediastinum, retroperitoneum, buttock, and perineum 3. Treatment is reserved for symptomatic lesions that cause pain, significant deformity, or threaten vital structures a. High-flow vascular malformations characterized by warmth, pain, bony destruction, discoloration and sometimes ulceration of the overlying skin 2. A working knowledge of the anatomy of the head and neck is crucial in the diagnosis and surgical treatment of these diseases. Control active bleeding by pressure, may need direct ligation in operating room or embolization in interventional radiology suite 2. Palpate facial skeleton for underlying bone pain and instability; rule out injury to facial nerve, parotid duct, etc. Wounds closed preferably less than 8 hours post-injury, but primary closure may be delayed up to 24 hours b. Physical examination for asymmetry, bone mobility, diplopia, extraocular muscle entrapment, sensory loss, malocclusion, local pain c. Once occlusion is aligned, work systematically, either "outside-in" (Gruss) or "inside-out" (Manson), establishing facial height, width, and projection by aligning key facial buttresses (open reduction) and plating of fractures (internal fixation) 2. Nasal bone fracture most common facial fracture (a) Septal hematoma can cause septal necrosis; must be drained immediately (b) May be corrected by closed reduction/manipulation and placement of external splint and Doyle splints (internal) ii. Le Fort fractures (Figure 3) 51 (a) Disrupts vertical maxillary buttresses: major areas of structural stability (i) Zygomaticomaxillary (ii) Nasomaxillary (iii) Pterygomaxillary (b) Treatment involves open reduction and internal fixation with miniplates to reestablish facial proportions and occlusion Figure 3. Usually more conservative with operative repair in this patient population, due to growing facial skeleton and developing dentition.
In the s e l o c a t i o n s the y a s s i s t i n r f o r ma t i o n o f t h er i a l a n d v e n t r i c u lm r m b r a n o u s p o r t i o n)p t a the at (ae se gastritis gurgling stomach buy generic florinef 0.1 mg on line, a t r i o v e n t r i c u l a r c a n a l s a n d v gastritis jelentese effective 0.1mg florinef, aav e st h e o r t i c a n d p u l m o n a r y c h a n n e l s gastritis or gastroenteritis generic florinef 0.1 mg overnight delivery. S e p t u m f o r ma t i o n b y t w o a c t i v e l y g r o w i n g r i d g e s t h a t 3 a p p r o a c h e a c h o the r u n t i l the yCf gastritis symptoms list safe florinef 0.1mg. S u c h a s e p t u m n e v e r c o mp l e t e l y s e p a r a t e s two cavities. T h e o the r ma n n e r i n w h i c h a s e p t u m i s f o r me d d o e s n o t i n v o l v e e n d o c a r d i a l c u s h i o n s. If, f o r e xa mp l e, a n a r r o w s t r i p o f t i s s u e i n the w a l l o f the a t r i u m o r v e n t r i c l e s h o u l d f a i l t o g r o w w h i l e a r e a s o n e a c h s i d e o f i t e xp a n d r a p i d l y, a n a r r o w r i d g e f o r ms b e t w e e n the t w o e xp a n d i n g pF irg i. E W h e n g r o w t h o f o t ns (the e xp a n d i n g p o r t i o n s c o n t i n u e s o n e i the r s i d e o f the n a r r o w p o r t i o n, the t w o w a l l s a p p r o a c h e a c h o the r a n d e v e n t u a l l y me r g e, f o r mi n g ia. It i s u s u a l l y c l o s e d secondarily by tissue contributed by neighboring proliferating tissues. Clinical Corre late s Endocardial Cushions and He art De fe cts B e c a u s e o f the i r k e y l o c a t i o n, a b n o r ma l i t i e s i n e n d o c a r d i a l c u s h i o n f o r ma t i o n c o n t r i b u t e t o ma n y c a r d i a c ma l f o r ma t i o n s, ia tc liu da n gv e n t r i c u l a r n r al i d s e p t a l d e f e c tas d d e f e c t s i n v o l v i n ggtrh e t v e s s e l(s. T h i s c r e s t i s the f i r s t p o reip tn mf the S t o uo p r i m u m(s e eF i g s. T h e t w o l i mb s o f t h i s s e p t u m e xt e n d A B toward the endocardial cushions in the atrioventricular canal. The opening between the l o w e r r i m o f the s e p t u m p r i mu m a n d the e n d o c a r d i a l c u s hs oin s i s the o it um p r i m u m(F i g. B W i t h f u r the r d e v e l o p me n t, e xt e n s i o n s o f the s u p e r i o r a n d) i n f e r i o r e n d o c a r d i a l c u s h i o n s g r o w a l o n g the e d g e o f the s e p t u m p r i mu m, c l o s i n g the o s t i u m p r i muF i g(. D B e f o r e c l o s u r e i s c o mp l e t e, h oc e lv e r, m we l d e a t hp r o d u c e s p e r f o r a t i o n s i n the u p p e r p o r t i o n o f the s e p t u m p r i mu m. C o a l e s c e n c e o f the s e p e r f o r a t i o n s f o r ms i uh e s e c u n d u m n s u r i n g f r e e ost t m, e b l o o d f l o w f r o m the r i g h t t o the l e f t p r i mi t i v ei ga t r i 2. When the left venous valve and the septum spurium fuse w i t h the r i g h t s i d e o f the s e p t u m s e c u n d u m, the f r e e c o n c a v e e d g e o f the s e p t u m s e c u n d u m b e g i n s t o o v e r l a p the o s t i u m s e c ug. In a b o u t 2 0 % o f c a s e s, f u s i o n o f the s e p t u m p r i mu m a n d s e p t u m s e c u n d u m i s i n c o mp l e t e, a n d a n a r r o w o b l i q u e c l e f t r e ma i n s b e t w e e n the t w o a t r i a. T h i s c o n d i t ip rn bs c a l l e d o oi e p a t e n c yo f the o v a l f o r a me n; i t d o e s n o t a l l o w i n t r a c a r d i a c s h u n t i n g o f b l o o d. Furthe r Diffe re ntiation of the Atria W h i l e the p r i mi t i v e r i g h t a t r i u m e n l a r g e s b y i n c o r p o r a t i o n o f the r i g h t s i n u s h o r n, the p r i mi t i v e l e f t a t r i u m i s l i k e w i s e e xp a n d i n g. In i t i a l l y, a s i n g l e e mb r y o n i c p u l m o n a r y v e id e v e l o p s a s a n o u t g r o w t h o f the p o s t e r i o r l e f t a t r i a l w a l l, j u s t t o n the l e f t o f the s e p t u m p r i mu m i(g. D u r i n g f u r the r d e v e l o p me n t, the p u l mo n a r y v e i n a n d i t s b r a n c h e s a r e i n c o r p o r a t e d i n t o the l e f t a t r i u m, f o r mi n goto the - a r g e sm h h l w a l l e dp a r t o f the a d u l t a t r i u m. Al t h o u g h i n i t i a l l y o n e v e i n e n t e r s the l e f t a t r i u m, u l t i ma t e l y f o u r p u l mo n a r y v e i n s F in t. In the f u l l y d e v e l o p e d h e a r t, the o r i g i n a l e mb r y o n i c l e f t a t r i u m i s r e p r e s e n t e d b y l i t t l e mo r e t h a n t ha b e c u l a t e d a t r i a l a p p e n,d wg el e the s mo o t h - w a l l e d p a r t re a hi o r i g i n a t e s f r o m the p u l mo n a r y v egn s 2. S e p t u m F o r m a t i o n i n the A t r i o ve n t r i c u l a r C a n a l At the e n d o f the f o u r t h w e e k, t w o me s e n c h y ma l c u sa tir i n s,etn the i c u l a r h o ov h r e ndocardial cushions pear at the superior and inferior borders of the, ap a t r i o v e n t r i c u l a r c a n a l Fs g s. B o t h the w a l l o f the r i g h t s i n u s h o r (bl ue)a n d the p u l mo n a r y v e r n s a r e i n c o r p o r a t e d i n t o the h e a r t n (i ed) t o f o r m the s mo o t h - w a l l e d p a r t s o f the a t r i a. T h e i n i t i a l c i r c u l a r o p e n i n g w i d e n s t r a n s v e r s e l y. In a d d i t i o n t o the s u p e r i o r a n d i n f e r i o r e n d o c a r d i a l c u s h i loa ts,r ah e t w o ne tl a t r i o v e n t r i c u l a r c u s h i a p p e a r o n the r i g h t a n d l e f t b o r d e r s o f t h ei gcsa n a l (ons F. T h e s u p e r i o r a n d i n f e r i o r c u s h i o n s, i n the me a n t i me, p r o j e c t) f u r the r i n t o the l u me n a n d f u s e, r e s u l t i n g i n a c o mp l e t e d i v i s i o n o f the c a n a l i n t o r i g h t a n d l e f t a t r i o v e n t r i c u l a r o r i f i c e s b y the e n d o f the i fg f t h 2w1 6 k (F i. At t h i s 7 s t a g e o f d e v e l o p me n t, b l o o d f r o m the a t r i a l c a v i t y e n t e r s the p r i mi t i v e l e f t v e n t r i c l e a s w e l l a s the p r i mi t i v e r i g h t v e n t r i c l.
Order florinef 0.1 mg without prescription. How to Make Cleansing Ginger Water With Many Health Benefits.
Roth et al [3] tested four different ionic and nonionic iodinated contrast media through 12 different-sized catheters at both human body (37o C) and room temperature (20o C) gastritis diet 321 order florinef on line amex, and measured the power injection pressure of each combination using a 7 mL injection at 3 mL/second with an electronic pressure transducer gastritis diagnosis florinef 0.1mg online. Busch et al [4] studied the iodine delivery rates of four different contrast media through five different catheters used for coronary angiography at power injections of 100 digestive gastritis through diet buy 0.1 mg florinef amex, 200 gastritis help buy cheap florinef 0.1mg on line, and 400 psi. The iodine delivery rate improved with increasing pressure, increasing iodine content (mg I/mL) and decreasing contrast media viscosity. Although the authors did not test the effect of extrinsic warming, they speculated that the reduction in viscosity associated with warming may be a method by which iodine delivery rates might be improved. They found that the degree of maximal enhancement within the ascending aorta, descending aorta, and pulmonary arteries was significantly greater (p = 0. They also found that group 1 patients reached 100 Hounsfield Units of enhancement within the ascending aorta significantly faster than group 2 patients (p = 0. However, their data was solely based on the test injection (not the diagnostic injection). Iodinated Contrast Media  Contrast Material Warming and Adverse Events Although there is good evidence that warming of contrast media changes the bolus kinetics and injection pressure of iodinated contrast media, there has been little evidence that it affects clinical adverse event rates in a meaningful way [10-12]. The authors were unable to show a significant difference, although their study was likely underpowered for a non-inferiority design. These groups were then compared with respect to their allergic-like and physiologic adverse events. In most instances, this is performed using an external incubator in which the bottles of contrast media are placed. The temperature of the device is typically kept at or near human body temperature (37o C). In addition to these stand-alone warming machines, there also exist warming "sleeves" that can be used to keep pre-warmed bottles (or syringes filled from pre-warmed bottles) of contrast media at a stable (warmed) temperature for approximately one hour or more in cases where the contrast media is removed from the warming device but not immediately injected. These sleeves can be a component to the power injector itself or can function independently. Although some institutions have discontinued the routine use of contrast media warmers for low-rate (< 5 mL/second), non- angiographic, noncardiac applications, there are little published data investigating what effect this may have on patient adverse events. Discontinuation of contrast media warming had no significant effect on the allergic-like reaction or extravasation rates of iopamidol 300. These results suggest that contrast media warming may not be needed for iopamidol 300, but may be needed for iopamidol 370 (and possibly other similarly viscous contrast media) if the primary goal is to minimize contrast media-related adverse events. However, the authors did note that there was no difference in clinical outcome between the warmed and non-warmed iopamidol 370 groups, likely because the vast majority of extravasation events and allergic-like reactions do not result in long-term morbidity or mortality. The authors did not have any data to permit evaluation of the effect of extrinsic contrast media warming on patient comfort or physiologic. Warming of Iodinated Contrast Media  Suggestions Based on the available literature, the validity of extrinsic warmers seems predicated on the intended outcome. Warming of Gadolinium-Based Contrast Media-Suggestions Gadolinium-based contrast media are administered at room temperature (15 to 30o C [59 to 86o F]) and according to package inserts, should not be externally warmed for routine clinical applications. Comparative rheology of low- and iso-osmolarity contrast agents at different temperatures. Non-ionic contrast media: a comparison of iodine delivery rates during manual injection angiography. Influence of radiographic contrast media viscosity to flow through coronary angiographic catheters. Iodine delivery rate in catheter angiography under pressure conditions in manual injection. Haemodynamic and rheological effects of contrast media: the role of viscosity and osmolality. Peripheral intravenous power injection of iodinated contrast media: the impact of temperature on maximum injection pressures at different cannula sizes. Frequency of anaphylactoid reactions during intravenous urography with radiographic contrast media at two different temperatures. Future investigations building on recent methodological advancements [3,4,7,9], are necessary to clarify the incidence and significance of this disease. Patients who have an elevated serum creatinine at baseline have a greater variance in daily serum creatinine measurements than those with a normal baseline serum creatinine [10]. Etiologic factors that have been suggested include renal hemodynamic changes (vasoconstriction) and direct tubular toxicity, among others [16-26]. Both osmotic and chemotoxic mechanisms may be involved, and some investigations suggest agent-specific chemotoxicity.
St. Augustine Humane Society | 1665 Old Moultrie Rd. | St. Augustine, FL 32084 PO Box 133, St. Augustine, FL 32085 | Phone (904) 829-2737 |info@staughumane.org
Hours of Operation: Mon. - Fri. 9:00am - 4:00pm Closed for Lunch Each Day: 12:30pm - 1:30pm
Open Sat. by Appointment Only for Grooming General Operations Closed: Sat. and Sun.