Co-Director, Campbell University School of Osteopathic Medicine
Prepare infants for breastfeeding; initiate and encourage frequent skin-to-skin holding if infant is clinically stable skin care x effective lurantal 10mg. Request lactation support consults to initiate breastfeeding as early as possible acne lotion generic lurantal 5 mg amex. This approach skin care di jakarta buy discount lurantal 30mg online, called "cue-based" feeding acne on buttocks buy 10mg lurantal with amex, should underlie oral nutrition, especially in preterm infants. Risk factors for overt and silent aspiration: long-term intubation, severe hypotonia, neurological issues. Lactation consultants are available for initiation and progression of breastfeeding. Occupational therapists will provide non-nutritive oral stimulation, bottle feeding assessments, bedside swallow assessments, transition to spoon feeding, and co-consult with speech pathologist for craniofacial disorders. Speech pathologists will evaluate for clinical signs of dysphagia or swallowing issues. The use of swallow function studies to evaluate feeding disorders should be carefully considered by the medical team due to the radiation exposure of this test and limited evidence of clinical correlation of findings. Some infants need more time to develop appropriate sucking patterns, to coordinate suckswallow-breathe, for catch-up breathing, and/or rest more frequently. Consider advancing the number of oral feedings per day if infant shows good feeding skills with no oral aversion and demonstrates adequate endurance, even if feedings are partially completed. Lactation support professionals are available to assist mothers with milk expression and breastfeeding. Encouraging frequent breast stimulation (every 3 hours or 7 to 8 times per day) in the first few weeks after birth to promote an adequate milk supply. Instruct parents on milk supplementation, formula preparation, and vitamin/mineral supplementation as indicated. Consultation with the lactation consultant will provide individualized feeding strategies to assist in progression of breastfeeds. Pre- and post-weights (1 gram of weight change = 1 mL of milk intake) provide an objective measure of milk transfer. Premature infants may receive transitional formula up to 6 to 9 months corrected age. Infants may demonstrate catch-up growth quickly after discharge and can be changed to a standard term formula at 48-52 weeks post-menstrual age if weight and length (for corrected gestational age), and weightfor-length are all at least at the 25% percentile for age. Continuously monitor nutritional status including intakes, growth, and biochemical indices as indicated. Infants who are less than 1500 grams at birth: o If infant is to be discharged on plain human milk, suggest up to 3 feedings per day with a premature transitional formula and the remainder as breastfeeding. Premature transitional formula (22 kcal/oz) is available as a liquid ready-to-feed. In addition to providing multivitamins and iron, it is recommended that infants be evaluated 2 to 4 weeks after discharge. Consider an Occupational Therapy consult to assess developmental appropriateness and to assist with solid food introduction along with caregivers and parents. Introduce single-ingredient baby foods one at a time and continue 3 to 5 days before introducing an additional new food.
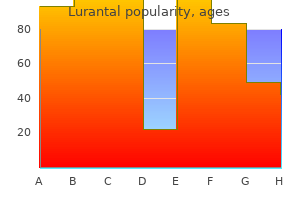
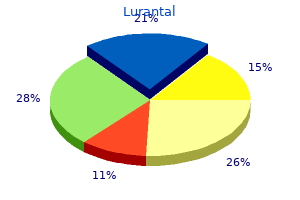
Fusoria (Wahoo). Lurantal.
Are there safety concerns?
Constipation, indigestion, water retention, and other conditions.
Dissemination and implementation research in health: translating science to practice acne 5dpo purchase 40 mg lurantal with amex. The sustainability of evidence-based interventions and practices in public health and health care skin care network buy lurantal 20 mg without a prescription. Shaping the context of health: a review of environmental and policy approaches in the prevention of chronic diseases skin care for acne lurantal 20 mg low price. Approaches to changing diet and physical activity should take into consideration healthenhancing environments acne zones and meaning buy 20 mg lurantal with visa, behaviour change communications, and systems change. Government regulatory measures, such as product nutrient specification, and fiscal interventions can be used to successfully affect dietary patterns, but industry opposition can influence the design of optimal programmes. Educational approaches and awareness-raising strategies can motivate and support people to change their behaviour, but their impact on dietary intake alone is small and may be lowest in vulnerable groups. Behavioural risk factors for cancer, such as diet and physical activity, are influenced by underlying social determinants, including economic, 506 political, environmental, and cultural factors; global efforts to reduce the burden of cancer need to take account of these social determinants in order to produce equitable changes in health and well-being [1]. Health services, including cancer screening programmes, can contribute to national efforts [3]. A comprehensive community approach to changing health behaviours has been demonstrated historically in the North Karelia Project in Finland, which showed significant reductions in cardiovascular outcomes, followed by reductions in cancer mortality, arising from "the correct theory base, comprehensive work with the population, and much hard work in the community" [4]. There is a growing evidence base on the impact of behaviour change communications and programmes, which include individual-level counselling by health professionals, education, and social support, such as demonstrated by the diabetes prevention programmes. However, these approaches tend to be intensive and may have low generalizability, especially in the most vulnerable communities [5]. There is now clear evidence that the greatest change in diet and physical activity across a population can be achieved when populationwide approaches, such as policy specification, are combined with individually targeted approaches. In addition, actions have to take account of the local context and the specific needs of the population (see Chapter 6. Natural experiments can provide useful evidence for intervention planning and policy development. Evidence from comprehensive community programmes suggests that a combination of behavioural theory, commitment, and national and local action are key factors in the design of programmes and policies. When implementing programmes that were successful in other regions, care needs to be taken to consider the local context and the specific needs of the population. Most research evidence has short- to medium-term outcomes, and more research is needed on programme sustainability, reach, and longterm outcomes to assess the impact of programmes and policies on cancer outcomes across all population groups. No single intervention can address the challenge of achieving healthy dietary patterns. It is clear that multiple factors, beyond personal decision-making, influence food choice and dietary patterns, including sociocultural background, lifestyle patterns, and economic and commercial pressures. Therefore, to achieve equitable, secure, sustainable, and optimal dietary intake, wider environmental factors need to be embraced in addition to individually focused approaches. For decades, nutrition programmes have focused primarily on behaviour change communications such as education programmes, food labelling information. These are considered to be important strategies to support people to practically implement advice, to help frame public understanding, and to generate support for healthy public policy, but their impact on dietary intake alone is small and may be lowest in vulnerable groups. More recently, many countries have developed voluntary codes of practice in conjunction with the food industry, for example reduction in sugar intake, but these have not been demonstrated to achieve desirable levels of change. Increasingly, it is recognized that government regulatory measures, such as product nutrient specification, and fiscal interventions can be used to successfully affect dietary patterns, but industry opposition can influence the design of optimal programmes. Actions by governments should be monitored, and accountability mechanisms should be in place at the local, national, and international levels [7]. Fiscal incentives and disincentives, such as food prices, subsidies, and financial rewards and penalties, are considered to be positive approaches in changing dietary behaviours, notably when implemented as part of an integrated package of mutually reinforcing activities, such as education and marketing. However, the level of financial impact needed to improve health outcomes needs to be carefully as508 sessed. The impact is likely to be greatest when regulatory rather than voluntary approaches are used [9]. Beverages Caloric beverages can make a significant contribution to excess energy intake and the development of weight gain, or may decrease appetite for more nutrient-dense foods, thus decreasing dietary quality.
One-stage versus two-stage exchange arthroplasty for infected total knee arthroplasty: a systematic review skin care 50s generic 40mg lurantal amex. Re-infection outcomes following one- and two-stage surgical revision of infected hip prosthesis: a systematic review and metaanalysis acne out buy genuine lurantal online. Comparison of one and two-stage revision of total hip arthroplasty complicated by infection: a Markov expected utility decision analysis acne qui se deplace et candidose discount lurantal master card. In patients with signs of systemic sepsis skin care tips for men buy lurantal with a visa, extensive comorbidities, infection with resistant organisms, culture-negative infections and poor soft tissue coverage, one-stage exchange arthroplasty may not be a good option. This popularity is mainly driven by a number of studies reporting comparable [1,2], if not better [3] outcomes of one-stage vs. Excellent outcomes for infectionfree survival are documented in the literature, especially where strict criteria for patient selection is met. It is important to note, however, that despite these reported findings, Jenny et al. In their series, only two patients with a sinus tract subsequently fell into their reinfection group [19]. Hence, it may be proposed that a discharging fistula is, in itself, not an absolute contraindication to one-stage exchange arthroplasty, a conclusion also drawn by Raut et al. It may be concluded that one-stage exchange arthroplasty remains a plausible option for the management of chronic prosthetic joint infections in a selected group of individuals with the prospect of promising results for infection-free survival of the revised prosthesis. Much of this evidence, however, is based upon analysis of prospective and retrospective observational studies. Furthermore, the fact that outcomes following one-stage exchange are affected by multiple factors, it is often difficult to assess the impact an individual criterion has. There is no doubt that stronger conclusions may be drawn in the future following results from established randomized controlled trials that are underway in the United Kingdom, United States, and elsewhere. In the meantime, we offer the following as indications and relative contraindications for onestage exchange arthroplasty. No radical debridement of infected soft tissues or bone is possible (for whatever reason). Despite these aforementioned studies, there still remains a lack of high-quality literature addressing the subject matter. Hence, in the absence of published randomized controlled trials, many of our conclusions have been drawn from a combination of retrospective and prospective cohort studies and systematic reviews of these. In this study, the microbiological profile appeared to play an important role onthe outcomes, with polymicrobial infections and atypical and gram-negative organisms being associated with a higher failure rate. Furthermore, in their series, only one of the five failures had documented negative culture [13]. Hence, it may be proposed that a lack of preoperative microbiological diagnosis may be considered a relative, rather than absolute, contraindication for one-stage exchange arthroplasty. Host and local factors have also been highlighted as important determinants of outcome of one-stage revision. Host profile in this series matched some of the indications criteria later set out by the International Consensus Group in 2013 to include the absence of systemic sepsis and gross tissue inflammation. Of the two reported cases of failure, both patients were noted to have severe immunosuppression [16]. Their series concluded better outcomes in terms of infection eradication with two-stage vs. They noted an absence of important bone defects intraoperatively (with only four cases requiring bone grafting) as a potential contributing factor to their successful outcomes [15]. The presence of soft tissue defects and sinus tracts also appear to have a negative impact on outcomes in some studies with a 27% reinfection rate (6 out of 22 cases) [18]. A multidisciplinary team approach to two-stage revision for the infected hip replacement. Outcomes of revision total hip replacement for infection after grading according to a standard protocol.
Tertiary care centre adherence to unified guidelines for management of periprosthetic joint infections: a gap analysis skin care secrets generic lurantal 5mg amex. Importance of selection and duration of antibiotic regimen in prosthetic joint infections treated with debridement and implant retention acne x-ray treatments lurantal 10 mg online. Early prosthetic joint infections treated with debridement and implant retention: 38 primary hip arthroplasties prospectively recorded and followed for median 4 years skin care salon lurantal 20mg for sale. Management of infection associated with total hip arthroplasty according to a treatment algorithm skin care jakarta barat generic lurantal 20 mg free shipping. The treatment and outcome of peri-prosthetic infection of the ankle: a single cohort-centre experience of 34 cases. Debridement and implant retention in the management of hip periprosthetic joint infection. Treatment strategies for periprosthetic infections after primary elbow arthroplasty. Debridement, antibiotics and implant retention in early periprosthetic joint infection after primary total hip arthroplasty: 88 percent survival after two years followup. Whenever possible, rifampin-based combinations should be used, but rifampin alone should never be used due to the rapid development of resistance. We recommend two to six weeks of parenteral antimicrobial therapy in combination with rifampin 300 to 450 mg orally twice a day, followed by rifampin plus a susceptible companion oral drug (such as trimethoprimsulfamethoxazole, ciprofloxacin or levofloxacin, a tetracycline, fusidic acid) depending on the individual tolerance, side effect profile and antimicrobial susceptibility testing [1,4,5]. Chronic oral suppression with trimethoprim-sulfamethoxazole, minocycline or doxycycline based on in vitro-susceptibilities and individual side effect profile and tolerance may be considered following the above regimens and should be reserved for patients who are unsuitable or refuse further surgical therapy. Clindamycinrifampin combination therapy for staphylococcal periprosthetic joint infections: a retrospective observational study. Outcome of debridement and retention in prosthetic joint infections by methicillin-resistant staphylococci, with special reference to rifampin and fusidic acid combination therapy. Evolution of Staphylococcus aureus under vancomycin selective pressure: the role of the small-colony variant phenotype. Daptomycin pharmacodynamics against Staphylococcus aureus hemB mutants displaying the small colony variant phenotype. Reduced glycopeptide and lipopeptide susceptibility in Staphylococcus aureus and the "seesaw effect": Taking advantage of the back door left open Antibiotic-resistant sub-populations of the pathogenic bacterium Staphylococcus aureus confer population-wide resistance. In fluoroquinolone-susceptible cases, the recommended antibiotic agent is a fluoroquinolone. Studies have been performed demonstrating the preferred antibiotic agent for treating these infections, but few relate to the preferred route, dose and duration of antibiotic treatment. The study demonstrated that the use of fluoroquinolones (in this study ciprofloxacin) was associated with the highest success rate of 79% (98 of 124), while the success in the remainder of the patients treated with other antibiotic regimen. The cohort of patients included in the study were mostly infected with Enterobacteriaceae spp. Several other smaller studies have been performed, supporting the beneficial effect of fluoroquinolones. All of these patients were initially treated with -lactam antibiotics intravenously, and 14 patients were subsequently treated with oral ciprofloxacin. Treatment failure occurred in two patients not treated with ciprofloxacin (median period of follow-up of 28 months). Whether a short or long treatment duration was associated with a respectively lower or higher cure rate was not described in most studies. No studies evaluated the dosage of antibiotic treatment and its relation to outcome. Time trends in the aetiology of prosthetic joint infections: a multicentre cohort study. Gram-negative prosthetic joint infection treated with debridement, prosthesis retention and antibiotic regimens including a fluoroquinolone. Long-term outcome of acute prosthetic joint infections due to gram-negative bacilli treated with retention of prosthesis. Drug treatments for prosthetic joint infections in the era of multidrug resistance.
20mg lurantal sale. Meagan Good Says She DOESN’T Ble@ch Her Skin.
St. Augustine Humane Society | 1665 Old Moultrie Rd. | St. Augustine, FL 32084 PO Box 133, St. Augustine, FL 32085 | Phone (904) 829-2737 |info@staughumane.org
Hours of Operation: Mon. - Fri. 9:00am - 4:00pm Closed for Lunch Each Day: 12:30pm - 1:30pm
Open Sat. by Appointment Only for Grooming General Operations Closed: Sat. and Sun.